
Source from Kelvin A. Power’s Facebook on November 11, 2019
Gamma-Glutamyl Transferase (GGT)၊ရုတ်တရက်အရမ်းမြင့်တက်လာတယ်။ ရောဂါသိသွားရင်တော့ကုရတာလွယ်ပါတယ်။စိုးရိမ်စရာမရှိပါဘူး။ အရင်တုံးကကို
Min Tha
ကသွေးစစ်ထားတာတွေလာပြပြီး(GGT)မြင့်နေလို့လာမေးထားပါတယ်။ပထမတစ်ခေါက်ကညာဘက်ရင်ညွန့်အောက်နားကထောက်နေသလိုဖြစ်ပြီးနာကျင်တဲ့အကြောင်းကိုပြည့်ပြည့်စုံစုံပြောမပြတော့(GGT)တွေမြင့်တက်နေတာကိုကြည့်ပြီး(Liver)ပျက်စီးနိုင်တယ်လို့ကျွန်တော်ခန့်မှန်းခဲ့ပါတယ်။ ဒါပေမဲ့နောက်တော့အသစ်ထပ်ပြီးသိရတာရှိလာပါတယ်။
—
ရက်တော်တော်ကြာတော့မှသူကဘာထပ်ပြောလဲဆိုတော့— (fastingကိုလည်းတစ်ပတ်၃ကြိမ်လုပ်ဖြစ်ပါတယ်ခင်ဗျာ…အဲ့လိုပြုလုပ်ပြီးရက်၂၀လောက်အကြာမှာညာဘက်ရင်ညွန့်အောက်နားကထောက်နေသလိုဖြစ်ပြီးချွေးစေးများပြန်လာပါတယ်…ခြေဖျားလက်ဖျားတွေလည်းအေးစက်လာပါတယ်…အဲ့လက္ခဏာတွေကဆရာ့ဆေးမသောက်မှီကလည်းမကြာခဏဆိုသလိုဖြစ်နေတာပါ…ခုတော့ဆေးစသောက်ပြီးရက်၂၀အကြာမှပြန်ဖြစ်တာ၃ရက်ဆက်တိုက်လောက်ရှိနေပါပြီ…ဖြစ်ချိန်များကလည်းအချိန်မတော်ညဘက်အိပ်နေချိန်များဖြစ်ပါတယ်…အဲ့လိုချိန်ဆိုအရမ်းခံရခက်ပါတယ်…ဘာအတွက်ကြောင့်များအဲ့လိုဖြစ်ရလည်းဆိုတာသိချင်လို့ပါခင်ဗျာ။
—–
သူအရင်ကတည်းကမကြာခဏညာဘက်ရင်ညွန့်အောက်နားကထောက်နေသလိုဖြစ်ပြီးမကြာခဏနာကျင်တဲ့အကြောင်းအခုမှပြည့်ပြည့်စုံစုံသိရတော့ကျွန်တော်တစ်မျိုးပြန်ပြင်ပြီးပြောချင်တယ်။(Liver)ပျက်စီးနေတာမဟုတ်နိုင်ပါဘူး။ပြည့်ပြည့်စုံစုံသိလာရတော့တမျိုးပြောင်းပြောပါရစေ။သတင်းကောင်းပါ။ (Liver)ကောင်းနေနိုင်ပါတယ်။
—
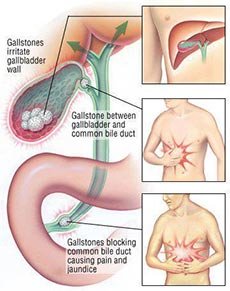
အခုဘာဖြစ်လဲဆိုတာသေသေချာချာပြောပြပါမယ်။(liver)ရဲ့အောက်နားလေးမှာ(Gallbladder)ဆိုတဲ့သည်းခြေအိတ်ကလေးတစ်ခုရှိပါတယ်။အဲဒီသည်းခြေအိတ်ထဲမှာ၊သည်းခြေရေ(bile)တွေကိုသိုလောင်ထားပေးပါတယ်။(Gallbladder)ဆိုတဲ့သည်းခြေအိတ်ကအဆီများများစားရင်သည်းခြေရေ(bile)တွေကိုအူလမ်းကြောင်းတွေထဲကိုညှစ်ထုတ်ပေးပြီးအဆီတွေကိုအစာချေဖျက်ဖို့ကူညီပေးရပါတယ်။
—
အဆီများများမစားတာကြာရင်၊သို့မဟုတ်အဆီကိုရှောင်ပြီးစားဖန်များလာရင်၊သည်းခြေအိတ်ထဲမှာရှိနေတဲ့သည်းခြေရေတွေကအူလမ်းကြောင်းထဲကိုထွက်မလာတော့ပါဘူး။သည်းခြေရည်တွေဟာထွက်မလာတာများလာရင်၊အနည်ထိုင်ပြီးတော့ခဲသွားတတ်ပါတယ်။ခဲသွားတဲ့သည်းခြေရည်အခဲတွေဟာကျောက်တုံးကလေးတွေလိုမာတဲ့အခဲကလေးတွေဖြစ်သွားတတ်ပါတယ်။
—
အဆီကိုပုံမှန်စားနေတဲ့လူတစ်ယောက်မှာသည်းခြေအိတ်ကသည်းခြေရည်အဟောင်းတွေကိုပုံမှန်ညှစ်ထုတ်လိုက်၊အသဲကနေအသစ်ထပ်ဝင်လာတဲ့သည်းခြေရည်အသစ်တွေကိုပြန်ပြီးသိုလှောင်ပေးထားလိုက်အမြဲလုပ်နေတော့။သည်းခြေရည်တွေကဟောင်းမသွားပဲအသစ်အသစ်ဖြစ်နေပြီးဘယ်တော့မှအနည်ထိုင်ပြီးခဲမသွားပါဘူး။
—
ဆီကိုမကျန်းမာဘူးဆိုတာသိလို့လျှော့စားလိုက်ရင်၊သည်းခြေအိတ်ကသည်းခြေရည်အဟောင်းတွေကိုညစ်မထုတ်ပေးပဲသိုလှောင်ထားလိုက်တော့၊သည်းခြေရည်အဟောင်းတွေဟာအချိန်ကြာတော့အနည်ထိုင်ပြီးအခဲကလေးတွေဖြစ်သွားပါတော့တယ်။အဲဒီလိုခဲလာပြီဆိုရင်ပြဿနာစတက်တော့တာပါပဲ။
—
ဒီလိုနဲ့သည်းခြေအိတ်ထဲမှာသည်းခြေရည်ခဲသွားလို့ဖြစ်လာတဲ့ကျောက်ခဲတုံးကလေးတွေဖြစ်ပေါ်လာပါတော့တယ်။နောက်ပိုင်းအစာစားလို့အဆီတွေပါလာရင်သည်းခြေအိတ်က၊သည်းခြေရည်တွေကိုပုံမှန်အတိုင်းညှစ်ထုတ်ပေးပါတယ်။ညှစ်ထုတ်ပေးလိုက်တော့သည်းခြေရည်တွေနဲ့အတူ၊ခဲနေတဲ့ကျောက်တုံးကလေးတွေလဲထွက်လာပါတော့တယ်။ထွက်လာတဲ့ကျောက်တုံးကလေးတွေဟာ(bile duct)လို့ခေါ်တဲ့သည်းခြေရည်ထုတ်ပေးတဲ့ပြွန်မှာလာပိတ်ပါလေရော။သည်းခြေပြွန်ပိတ်တော့အသဲကအူလမ်းကြောင်းထဲကိုသည်းခြေရည်တွေပြည့်ပြည့်ဝဝမထုတ်လွတ်နိုင်တော့ဘူး။
—
သည်းခြေရည်ခဲနေတဲ့ကျောက်တုံးလေးတွေသည်းခြေပြွန်အတွင်းမှာပိတ်မိနေပြီးသူတို့နဲ့ထိခိုက်ပွတ်တိုက်မိလို့ပြွန်အတွင်းနံရံတွေပွန်းပဲ့သွားလို့သည်းခြေပြွန်အတွင်းမှာအနာဒဏ်ရာဖြစ်ပြီးရောင်လာပါတော့တယ်။ရောင်တော့လမ်းကြောင်းပိုကျဉ်းလာ၊ပိုပိတ်လာပါတော့တယ်။သည်းခြေပြွန်ထိခိုက်မိတယ်။ဒဏ်ရာအနာတရဖြစ်တယ်။ရောင်လာတယ်ဆိုရင်(GGT)တွေရုတ်တရက်မြင့်တက်လာသလိုအသဲကသည်းခြေရည်ထုတ်လွတ်တဲ့လမ်းကြောင်းရုတ်တရက်ပိတ်နေရင်လဲ၊အသည်းကအညစ်အကြေးအဆိပ်အတောက်တွေကောင်းကောင်းမစွန့်ထုတ်နိုင်တော့လို့အသဲကြောင့်လဲ(GGT)တွေရုတ်တရက်မြင့်တက်လာတတ်ပါတယ်။
—
(GGT)တွေအများကြီးရုတ်တရက်တက်လာပြီး။မကြာခဏညာဘက်ရင်ညွန့်အောက်နားကထောက်နေသလိုဖြစ်ပြီးမကြာခဏနာကျင်နေတယ်ဆိုရင်တော့သည်းခြေပြွန်ပိတ်တယ်ဆိုတာ(၉၅%)လောက်သေချာပါတယ်။အသဲပျက်စီးဖို့ရာခိုင်နုန်းကတော့(၅%)လောက်ပဲရှိပါတယ်။အသဲပျက်စီးလို့(GGT)တက်တာမဟုတ်ပါဘူး။အစိုးရိမ်မလွန်ပါနဲ့။သည်းခြေပြွန်ပိတ်တာဟာအနေရအထိုင်ရခက်တယ်နာကျင်တတ်တယ်ဆိုပေမဲ့အသက်အန္တရာယ်တော့ရုတ်တရက်ကြီးမဖြစ်နိုင်ပါဘူး။အသဲကရုတ်တရက်ကြီးပျက်စီးသွားတယ်ဆိုရင်တော့အန္တရာယ်ရှိပါတယ်။
—
ဒီထက်ပိုပြီးသေချာအောင်လို့ကို
Min Tha
ကိုသွေးထဲမှာရှိနေတဲ့(ALT) (AST) (ALP)တွေကိုပါထပ်တိုင်းကြည့်စေချင်ပါတယ်။တစ်ကယ်လို့(GGT)တွေလဲတက်တယ်။(ALT) (AST) (ALP)တွေလဲလိုက်တက်နေတယ်ဆိုရင်တော့အသဲပျက်စီးနိုင်လို့စိုးရိမ်ရပါတယ်။
—
တစ်ကယ်လို့(GGT)တစ်ခုတည်းတက်နေပြီး။(ALT) (AST) (ALP)တွေလိုက်မတက်ဘူးဆိုရင်တော့သည်းခြေရည်ထုတ်တဲ့ပြွန်ကလေးထဲမှာသည်းခြေကျောက်ခဲတွေပိတ်နေပြီဆိုတာကိုတိတိကျကျပြောနိုင်ပါတယ်။မကြာခဏညာဘက်ရင်ညွန့်အောက်နားကထောက်နေသလိုဖြစ်ပြီးမကြာခဏနာကျင်နေတယ်။မတ်တပ်ရပ်နေတဲ့အချိန်၊ထိုင်နေတဲ့အချိန်တွေမှာသိပ်မဖြစ်ပဲလှဲအိပ်နေတဲ့အချိန်မှာပိုပြီးဖြစ်တတ်တယ်ဆိုရင်တော့၊(GGT)တွေတက်နေတာဟာအသဲရောဂါမဟုတ်တော့ပဲ။သည်းခြေပြွန်မှာသည်းခြေကျောက်တုံးကလေးတွေပိတ်နေတာအလွန်သေချာပါတယ်။
—
အသဲပျက်စီးနေပြီဆိုရင်တော့အလွန်အန္တရာယ်ကြီးပါတယ်။သည်းခြေပြွန်မှာကျောက်တုံးပိတ်တာကရေရှည်တော့မကောင်းပေမဲ့လောလောလတ်လတ်တော့အသက်အန္တရာယ်မဖြစ်နိုင်သေးပါဘူး။အသဲပျက်စီးတာလောက်ကြောက်စရာမကောင်းပါဘူး။မစိုးရိမ်ပါနဲ့စိတ်အေးအေးထားပါ။ (ALT)(SLT) (ALP)တိုင်းပြီးကျွန်တော့်ကိုပြန်ပြောပြပါ။
—
ဒီပို့စ်ကိုလူသိရှင်ကြားတင်ပေးလိုက်တာဟာလဲ။အလားတူရောဂါမျိုးတခြားလူတွေမှာလဲဖြစ်တတ်ကြလို့ဘာဖြစ်တယ်ဆိုတာစောစောစီးစီးတိတိကျကျသိပြီး၊အနာသိဆေးရှိကုသနိုင်အောင်အကျိုးကိုမျှော်ကိုးပြီးတင်ပေးလိုက်တာပါ။
—
အထူးမှတ်ချက်။(GGT)ကအသဲပျက်စီးရင်မြင့်တက်လာတတ်တဲ့အင်ဇိုင်းဆိုတာကတော့မှန်ပါတယ်။ဒါပေမဲ့နှလုံးသွေးကြောတွေ၊တခြားအင်္ဂါအစိတ်အပိုင်းတွေ၊ပြွန်တွေ၊ထိခိုက်ပျက်စီးတယ်၊ရောင်ကိုင်းဒဏ်ရာရတယ်ဆိုရင်လဲ(GGT)တွေတက်လာတတ်ပါတယ်။ဒါကြောင့်မို့(GGT)တက်နေတာတခုတည်းနဲ့တော့တိတိကျကျသေချာမပြောနိုင်ပါဘူး။
(၁)(GGT)တွေတက်ပြီး၊(TG)တွေလဲများနေတယ်(HDL)တွေလဲသိပ်နည်းနေတယ်ဆိုရင်နှလုံးထိခိုက်ဖွယ်ရာရှိပါတယ်။
(၂)(GGT)ရော(ALT) (AST) (ALP)ရောမြင့်တက်နေပြီဆိုရင်အသဲဆိုတာရာနုန်းပြည့်နှီးပါးသေချာပါတယ်။
(၃)(GGT)မြင့်တက်ပြီး၊(ALT),(AST), (ALP),(TG),(HDL)တွေပုံမှန်ဆိုရင်တော့အသဲရောနှလုံးရောမစိုးရိမ်ရပါဘူး။မကြာခဏညာဘက်ရင်ညွန့်အောက်နားကထောက်နေသလိုဖြစ်ပြီးမကြာခဏနာကျင်နေတယ်ဆိုရင်တော့သည်းခြေပြွန်ပိတ်တာတစ်ခုပဲဖြစ်နိုင်ပါတယ်။ညဖက်လဲှအိပ်နေမှဖြစ်တယ်ဆိုရင်ပိုပြီးသေချာပါတယ်။သည်းခြေအိတ်ထဲမှာသည်းခြေကျောက်ခဲလေးတွေရှိချင်လဲရှိနေဦးမယ်။သည်းခြေကျောက်တွေမရှိတော့ပဲထွက်သွားပြီးသည်းခြေပြွန်အနာဖြစ်ပြီးဆက်ရောင်နေတာလဲဖြစ်ချင်ဖြစ်နိုင်ပါတယ်။သေချာစစ်ဆေးသင့်ပါတယ်။
—
သည်းခြေရည်ထွက်တဲ့သည်းခြေပြွန်ပိတ်တယ်။ဒါမှမဟုတ်သည်းခြေပြွန်အနာဖြစ်ပြီးရောင်နေတယ်ဆိုရင်(GGT)ပက်ပက်စက်စက်ကိုချက်ချင်းတက်လာပါတယ်။သည်းခြေပြွန်ပြန်ပွင့်သွားပြီ၊အနာလဲမရှိတော့ဘူး၊အရောင်ကျသွားပြီဆိုရင်(GGT)ပြန်ကျသွားပါတယ်။ဆိုလိုချင်တာကအတက်မြန်အကျမြန်တယ်လို့ပြောချင်တာပါ။ဘယ်လောက်အတက်အကျမြန်သလဲဆိုရင်၊ဥပမာအရက်မှုးအောင်သောက်လိုက်ရင်လဲ(GGT)ချက်ချင်းတက်ပါတယ်။အမှုးပြေသွားပြီး(၃)ရက်(၄)ရက်လောက်ဆက်မသောက်ရင်ပြန်ကျလာပါတယ်။(GGT)အတက်အကျမြန်တဲ့သဘောကိုပြောပြတာပါ၊ကာယကံရှင်လူနာအရက်မသောက်ဘူးဆိုတာကိုလဲနားလည်ထားပါတယ်။(GGT)တက်တိုင်းမစိုးရိမ်ပါနဲ့(ALT),(AST),(ALP)တိုင်းပြီးမှပြန်ပြောပြပါ။(GGT)တက်ပြီး(ALT),(AST) (ALP)လိုက်ပြီးမတက်ရင်အသဲကောင်းနေပါတယ်။
အားလုံးကျန်းမာပါစေ။
Kelvin A Power
———————
1. Green RM, Flamm S. AGA technical review on the evaluation of liver chemistry tests. Gastroenterology 2002;123(4):1367-84. [PubMed]
2. Burkitt HG, Young B, Heath JW. Wheater’s functional histology: a text and colour atlas. 3rd ed. Edinburgh: Churchill Livingston, 1993.
3. Worobetz L, Hilsden R, Shaffer E, Simon J Pare P, Scully L, et al. The liver. In Thomson BR, Shaffer EA, editors. First Principles of Gastroenterology. 2nd ed. University of Toronto Press: Toronto; 1994.
4. Dufour DR, Lott JA, Nolte FS, Gretch DR, Koff RS, Seeff LB. Diagnosis and monitoring of hepatic injury. I. Performance characteristics of laboratory tests. Clin Chem 2000;46(12):2027-49. [PubMed]
5. Dufour DR, Lott JA, Nolte FS, Gretch DR, Koff RS, Seeff LB. Diagnosis and monitoring of hepatic injury. II. Recommendations for use of laboratory tests in screening, diagnosis, and monitoring. Clin Chem 2000;46(12):2050-68. [PubMed]
6. Gholson CF, Morgan K, Catinis G, Favrot D, Taylor B, Gonzalez E, et al. Chronic hepatitis C with normal aminotransferase levels: a clinical histologic study. Am J Gastroenterol 1997;92(10):1788-92. [PubMed]
7. Mofrad P, Contos MJ, Haque M, Sargeant C, Fisher RA, Luketic VA, et al. Clinical and histologic spectrum of nonalcoholic fatty liver disease associated with normal ALT values. Hepatology 2003;37(6):1286-92. [PubMed]
8. Dufour DR. Effects of habitual exercise on routine laboratory tests [abstract]. Clin Chem 1998;44 (Suppl 6):A136.
9. Narjes H, Nehmiz G. Effect of hospitalisation on liver enzymes in healthy subjects. Eur J Clin Pharmacol 2000;56(4):329-33. [PubMed]
10. Whitehead MW, Hawkes ND, Hainsworth I, Kingham JGC. A prospective study of the causes of notably raised aspartate aminotransferase of liver origin. Gut 1999;45(1):129-33. [PMC free article] [PubMed]
11. Chadha MS, Walimbe AM, Chobe LP, Arankalle VA. Comparison of etiology of sporadic acute and fulminant viral hepatitis in hospitalized patients in Pune, India during 1978-81 and 1994-97. Indian J Gastroenterol 2003; 22 (1): 11 -5. [PubMed]
12. Feld JJ, Heathcote EJ. Epidemiology of autoimmune liver disease. J Gastroenterol Hepatol 2003;18(10):1118-28. [PubMed]
13. Merryweather-Clarke AT, Pointon JJ, Shearman JD, Robson KJ. Global prevalence of putative haemochromatosis mutations. J Med Genet 1997; 34 (4): 275-8. [PMC free article] [PubMed]
14. Barton JC, Acton RT. Inheritance of two HFE mutations in African Americans: cases with hemochromatosis phenotypes and estimates of hemochromatosis phenotype frequency. Genet Med 2001;3(4):294-300. [PubMed]
15. Roberts EA, Schilsky ML. A practice guideline on Wilson disease. Hepatology 2003;37(6):1475-92. [PubMed]
16. Lee WM. Drug-induced hepatotoxicity. N Engl J Med 2003;349(5):474-85. [PubMed]
17. Fogden E, Neuberger J. Alternative medicines and the liver. Liver Int 2003; 23 (4): 213-20. [PubMed]
18. Vanderlinde RE. Review of pyridoxal phosphate and the transaminases in liver disease. Ann Clin Lab Sci 1986;16(2):79-93. [PubMed]
19. Cohen JA, Kaplan MM. The SGOT/SGPT ratio — an indicator of alcoholic liver disease. Dig Dis Sci 1979;24(11):835-8. [PubMed]
20. Diehl AM, Potter J, Boitnott J, Van Duyn MA, Herlong HF, Mezey E. Relationship between pyridoxal 5′-phosphate deficiency and aminotransferase levels in alcoholic hepatitis. Gastroenterology 1984;86(4):632-6. [PubMed]
21. Wroblewski F. The clinical significance of alterations in transaminase activities of serum and other body fluids. Adv Clin Chem 1958;1(2):313-51. [PubMed]
22. Rej R. Aminotransferases in disease. Clin Lab Med 1989;9(4):667-87. [PubMed]
23. Kamimoto Y, Horiuchi S, Tanase S, Morino Y. Plasma clearance of intravenously injected aspartate aminotransferase isozymes: evidence for preferential uptake by sinusoidal liver cells. Hepatology 1985;5(3):367-75. [PubMed]
24. Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. N Engl J Med 2000;342(17): 1266-71. [PubMed]
25. Gopal DV, Rosen HR. Abnormal findings on liver function tests. Postgrad Med 2000;107(2):100-14. [PubMed]
26. Rozen P, Korn RJ, Zimmerman HJ. Computer analysis of liver function tests and their interrelationship in 347 cases of viral hepatitis. Isr Med Sci 1970; 6 (1): 67 -79. [PubMed]
27. Dufour DR, Teot L. Laboratory identification of ischemic hepatitis (shock liver) [abstract]. Clin Chem 1988;34:A1287.
28. Seeto RK, Fenn B, Rockey DC. Ischemic hepatitis: clinical presentation and pathogenesis. Am J Med 2000;109(2):109-13. [PubMed]
29. Singer AJ, Carracio TR, Mofenson HC. The temporal profile of increased transaminase levels in patients with acetaminophen-induced liver dysfunction. Ann Emerg Med 1995;26(1):49-53. [PubMed]
30. Fuchs S, Bogomolski-Yahalom V, Paltiel O, Ackerman Z. Ischemic hepatitis: clinical and laboratory observations of 34 patients. J Clin Gastroenterol 1998; 26 (3):183-6. [PubMed]
31. Clermont RJ, Chalmers TC. The transaminase tests in liver disease. Medicine 1967; 46(2):197-207. [PubMed]
32. Marcellin P. Hepatitis C: the clinical spectrum of the disease. J Hepatol 1999; 31 (Suppl 1):9-16. [PubMed]
33. Geller SA. Hepatitis B and hepatitis C. Clin Liver Dis 2002;6(2):317-34. [PubMed]
34. Wedemeyer H, Jackel E, Wiegand J, Cornberg M, Manns MP. Whom? When? How? Another piece of evidence for early treatment of acute hepatitis C. Hepatology 2004;39(5):1201-3. [PubMed]
35. Shad JA, Chinn CG, Brann OS. Acute hepatitis after ingestion of herbs. South Med J 1999;92(11):1095-7. [PubMed]
36. O’Grady JG. Acute liver failure. In: Comprehensive Clinical Hepatology. O’Grady JG, Lake JR, Howdle PD, editors. Mosby:London, 2000. p. 16.1-16.13.
37. Sellers EM, Freedman F. Treatment of acetaminophen poisoning. CMAJ 1981; 125(8):827-9. [PMC free article] [PubMed]
38. Mendenhall CL. Alcoholic hepatitis. The VA Cooperative Study Group on Alcoholic Hepatitis. ClinGastroenterol 1981;10(2): 417-41. [PubMed]
39. Goldberg S, Mendenhall C, Anderson S, Garcia-Pont P, Kiernan T, Seeff L, et al. VA Cooperative Study on Alcoholic Hepatitis. IV. The significance of clinically mild alcoholic hepatitis-describing the population with minimal hyperbilirubinemia. Am J Gastroenterol 1986;81(11):1029-34. [PubMed]
40. Krawitt EL. Autoimmune hepatitis. N Engl J Med 1996;334(14):897-903. [PubMed]
41. Kessler WR, Cummings OW, Eckert G, Chalasani N, Lumeng L, Kuo PY. Fulminant hepatic failure as the initial presentation of acute autoimmune hepatitis. Clin Gastroenterol Hepatol 2004;2(7):625-31. [PubMed]
42. Alvarez F, Berg PA, Bianchi FB, Bianchi L, Burroughs AK, Cancado EL, et al. International Autoimmune Hepatitis Group Report: review of criteria for diagnosis of autoimmune hepatitis. J Hepatol 1999;31(5):929-38. [PubMed]
43. Forston WC, Tedesco FJ, Stames EC, Shaw CT. Marked elevation of serum transaminase activity associated with extrahepatic biliary tract disease. J Clin Gastroenterol 1985;7(6):502-5. [PubMed]
44. Anciaux ML, Pelletier AG, Attali P, Meduri B, Liguory C, Etienne JP. Prospective study of clinical and biochemical features of symptomatic choledocolithiasis. Dig Dis Sci 1986;31:449-53. [PubMed]
45. Ferenci P, Caca K, Loudianos G, Mieli-Vergani G, Tanner S, Sternlieb I, et al. Diagnosis and phenotypic classification of Wilson disease. Liver Int 2003; 23 (3):139-42. [PubMed]
46. Maria VA, Victorino RM. Development and validation of a clinical scale for the diagnosis of drug-induced hepatitis. Hepatology 1997;26(3):664-9. [PubMed]
47. Aithal GP, Rawlins MD, Day CP. Clinical diagnostic scale: a useful tool in the evaluation of suspected hepatotoxic adverse drug reactions. J Hepatol 2000;33(6);949-52. [PubMed]
48. Harrison SA, Kadakia S, Lang KA, Schenker S. Nonalcoholic steatohepatitis: what we know in the new millenium. Am J Gastroenterol 2002;97(11):2714-24. [PubMed]
49. Brunt EM. Nonalcoholic steatohepatitis. Semin Liver Dis 2004;24(1):3-20. [PubMed]
50. Angulo P, Keach JC, Batts KP, Lindor KD. Independent predictors of liver fibrosis in patients with nonalcoholic steatohepatitis. Hepatology 1999; 30 (6): 1356-62. [PubMed]
51. Matteoni CA, Younossi ZM, Gramlich T, Boparai N, Liu YC, Mc-Cullogh AJ. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology 1999;116(6):1413-9. [PubMed]
52. Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J Viral Hepat 2004; 11 (2): 97-107. [PubMed]
53. The Global Burden Of Hepatitis C Working Group. Global burden of disease (GBD) for hepatitis C. J Clin Pharmacol 2004;44 (1):20-9. [PubMed]
54. Mele A, Spada E, Sagliocca L, Ragni P, Tosti ME, Gallo G, et al. Risk of parenterally transmitted hepatitis following exposure to surgery or other invasive procedures: results from the hepatitis surveillance system in Italy. J Hepatol 2001;35(2):284-9. [PubMed]
55. Memon MI, Memon MA. Hepatitis C: An epidemiological review. J Viral Hepat 2002;9(2):84-100. [PubMed]
56. Williams AL, Hoofnagle JH. Ratio of serum aspartate to alanine aminotransferase in chronic hepatitis. Relationship to cirrhosis. Gastroenterology 1988; 95 (3): 734-9. [PubMed]
57. Giannini E, Botta F, Fasoli A, Ceppa P, Risso D, Lantieri PB, et al. Progressive liver functional impairment is associated with an increase in AST/ALT ratio. Dig Dis Sci 1999;44(6):1249-53. [PubMed]
58. Giannini E, Risso D, Botta F, Chiarbonello B, Fasoli A, Malfatti F, et al. Validity and clinical utility of the aspartate aminotransferase-alanine aminotransferase ratio in assessing disease severity and prognosis in patients with hepatitis C virus-related chronic liver disease. Arch Intern Med 2003;163(2):218-24. [PubMed]
59. Giannini E, Botta F, Testa E, Romagnoli P, Polegato S, Malfatti F, et al. The 1-year and 3-month prognostic utility of the AST/ALT ratio and model for end-stage liver disease score in patients with viral liver cirrhosis. Am J Gastroenterol 2002;97(11):2855-60. [PubMed]
60. Tavill AS. Diagnosis and management of Hemochromatosis. Hepatology 2001; 33 (5):1321-8. [PubMed]
61. Czaja AJ. Natural history, clinical features, and treatment of autoimmune hepatitis. Semin Liver Dis 1984;4(1):1-12. [PubMed]
62. Morrison ED, Kowdley KV. Genetic liver disease in adults: early recognition of the three most common causes. Postgrad Med 2000;107(2):147-59. [PubMed]
63. Abdo A, Meddings J, Swain M. Liver abnormalities in celiac disease. Clin Gastroenterol Hepatol 2004;2(2):107-12. [PubMed]
64. Farrell RJ, Kelly CP. Diagnosis of celiac sprue. Am J Gastroenterol 2001; 96 (12): 3237-46. [PubMed]
65. Fishman WH. Alkaline phosphatase isoenzymes: recent progress. Clin Biochem 1990;23(2):99-104. [PubMed]
66. Moss DW. Physiochemical and pathophysiological factors in the release of membrane-bound alkaline phosphatase from cells. Clin Chim Acta 1997; 257 (1): 133-40. [PubMed]
67. Schlaeger R, Haux D, Kattermann R. Studies on the mechanism of the increase in serum alkaline phosphatase activity in cholestasis: significance of the hepatic bile acid concentration for the leakage of alkaline phosphatase from rat liver. Enzyme 1982;28(1):3-13. [PubMed]
68. Velayudham LS, Farrell GC. Drug-induced cholestasis. Expert Opin Drug Saf 2003;2(3):287-304. [PubMed]
69. Ponsioen CI, Tytgat GN. Primary sclerosing cholangitis: a clinical review. Am J Gastroenterol 1998;93(4):515-23. [PubMed]
70. Heathcote J. Update on primary biliary cirrhosis. Can J Gastroenterol 2000; 14 (1): 43-8. [PubMed]
71. Poupon R. Autoimmune overlapping syndromes. Clin Liver Dis 2003; 7 (4): 865-78. [PubMed]
72. Bonnand AM, Heathcote EJ, Lindor KD, Poupon RE. Clinical significance of serum bilirubin levels under ursodeoxycholic acid therapy in patients with primary biliary cirrhosis. Hepatology 1999;29(1):34-43. [PubMed]
73. Kim WR, Therneau TM, Wiesner RH, Poterucha JJ, Benson JT, Malinchoc M, et al. A revised natural history model for primary sclerosing cholangitis. Mayo Clin Proc 2000;75(7):688-94. [PubMed]
74. Rosalki SB, Tarlow D, Rau D. Plasma gamma-glutamyl transpeptidase elevation in patients receiving enzyme-inducing drugs. Lancet 1971;2:376-7. [PubMed]
75. McCullough AJ. Update on nonalcoholic fatty liver disease. J Clin Gastroenterol 2002;34(3):255-62. [PubMed]
76. Giannini E, Botta F, Fasoli A, Romagnoli P, Mastracci L, Ceppa P, et al. Increased levels of gammaGT suggest the presence of bile duct lesions in patients with chronic hepatitis C: absence of influence of HCV genotype, HCV-RNA serum levels, and HGV infection on this histological damage. Dig Dis Sci 2001;46(3):524-9. [PubMed]
77. Berk PD, Noyer C. Clinical chemistry and physiology of bilirubin. Semin Liver Dis 1994; 4(4):346-55.
78. Fevery J, Blanckaert N. What can we learn from analysis of serum bilirubin. J Hepatol 1986;2(1):113-21. [PubMed]
79. Bosma PJ, Chowdury JR, Bakker C, Gantla S, de Boer A, Oostra BA, et al. The genetic bases of the reduced expression of bilirubin UDP-glucuronosyltransferase 1 in Gilbert’s syndrome. N Engl J Med 1995;333(18):1171-5. [PubMed]
80. Thomsen HF, Hardt F, Juhl E. Diagnosis of Gilbert’s syndrome. Scand J Gastroenterol 1981;16(5):699-703. [PubMed]
81. Van Hootegem P, Fevery J, Blanckaert N. Serum bilirubins in hepatobiliary disease: comparison with other liver function tests and changes in the postobstructive period. Hepatology 1985;5(1):112-7. [PubMed]
82. Doumas BT, Peters T. Serum and urine albumin: a progress report on their measurement and clinical significance. Clin Chim Acta 1997;258(1):3-20. [PubMed]
83. Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg 1973; 60 (8): 646-9. [PubMed]
84. Bonis PA, Tong MJ, Blatt LM, Conrad A, Griffith JL. A predictive model for the development of hepatocellular carcinoma, liver failure, or liver transplantation for patients presenting to clinic with chronic hepatitis C. Am J Gastroenterol 1999;94(6):1605-12. [PubMed]
85. Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Therneau TM, Kosberg CL, et al. A model to predict survival in patients with end-stage liver disease. Hepatology 2001;33(2):464-70. [PubMed]
86. Botta F, Giannini E, Romagnoli P, Fasoli A, Malfatti F, Chiarbonello B, et al. MELD scoring system is useful for predicting prognosis in patients with liver cirrhosis and is correlated with residual liver function: a European study. Gut 2003;52(1):134-9. [PMC free article] [PubMed]
87. Jalan R, Hayes PC. Review article: quantitative tests of liver function. Aliment Pharmacol Ther 1995;9(3):263-70. [PubMed]