Source from Kelvin A. Power’s Facebook on August 8, 2019
ကျွန်တော်တို့တွေဟာဒီခေတ်ဆေးပညာကိုအလွန်အားကိုးယုံကြည်ခဲ့ကြသလိုတိုင်းပြည်အသီးသီးကလဲဆရာဝန်တွေ၊အသိပညာရှင်အတတ်ပညာရှင်တွေ၊ပေါ်ထွက်လာနိုင်ဖို့ငွေကြေးတွေအမြောက်အများသုံးစွဲခဲ့ကြပါတယ်။အနောက်နိုင်ငံတွေမှာလဲဒေါ်လာဘီလျှံနဲ့ချီကိုလူသားတွေမှာဖြစ်ပွားနေတဲ့နှလုံးရောဂါ၊ဆီးချိုရောဂါ၊ကင်ဆာရောဂါအစရှိတဲ့ရောဂါဆိုးတွေကိုကုသနိုင်ဖို့်အတွက်သုသေသနလုပ်ငန်းတွေမှာသုံးစွဲခဲ့ကြပါတယ်။(၂၀)ရာစုနစ်ကတည်းပရဟိတစိတ်ဓါတ်ရှိတဲ့လူတွေဟာရည်ရွယ်ချက်ကြီးကြီးမားမားနဲ့လာမယ့်(၂၁)ရာစုနစ်မျိုးဆက်သစ်တွေမှာသူတို့လက်ထက်ကခံစားခဲ့ရတဲ့ရောဂါဆိုးတွေထပ်ပြီးမခံစားရအောင်(လူတိုင်းကျန်းမာသက္ကရာဇ်နှစ်ထောင်မှာ)ဆိုတဲ့ဆောင်ပုဒ်တခုကိုအောင်လံလို့သတ်မှတ်လွှင့်ထူထားကြပြီးတော့သုတေသနလုပ်ငန်းတွေမှာငွေတွေပုံပြီးလှူဒါန်းခဲ့ကြပါတယ်။ဒါပေမဲ့၊အခုတော့အရင်းရှင်စနစ်ဆိုးရဲ့အောက်မှာကျွန်တော်တို့လူသားတွေအားကိုးတကြီးနဲ့ရင်းနီးမြုပ်နံှစိုက်ပျိုးခဲ့ရတဲ့ခေတ်ပေါ်ဆေးပညာဟာလုံးဝကျဆုံးသွားခဲ့ရပါပြီ။ကျွန်တော်တို့ရဲ့(လူတိုင်းကျန်းမာသက္ကရာဇ်နစ်ထောင်မှာ)ဆိုတဲ့အောင်လံလဲလဲှခဲ့ရပါပြီ။တကယ့်လက်တွေ့မှာတော့ကျွန်တော်တို့ရဲ့မျှော်လင့်ချက်တွေပျောက်ဆုံးပျက်စီးသွားခဲ့ရလို့အင်မတန်မှဝမ်းနည်းစရာကောင်းပါတယ်။အခုတော့တိုင်ထိပ်မှာ(လူတိုင်းရောဂါ၊သက္ကရာဇ်နစ်ထောင်မှာ)ဆိုတဲ့အရင်းရှင်တို့ရဲ့အောင်လံလွှင့်ထူနိုင်ခဲ့ပါပြီ။
———————-
ကျွန်တော်တို့ရဲ့သူငယ်ချင်းမိတ်ဆွေတွေ၊ကျွန်တော်တို့ရဲ့မိဘဆွေမျိုးမောင်နှမတွေဟာနေ့စဉ်နေ့တိုင်းတစ်ယောက်ပြီးတစ်ယောက်ရောဂါဆိုးတွေအောက်မှာအသက်ပေးပြီးသေဆုံးနေကြရပါပြီ။ကျွန်တော်တို့တွေသူတို့အတွက်ဘာတွေလုပ်ပေးနိုင်ကြမလဲ?။သူတို့တွေဖြစ်နေတာကိုငါနဲ့မဆိုင်သေးဘူး၊ငါ့အလှည့်လဲမကျသေးဘူး၊အေးဆေးပဲဆိုပြီးကိုယ့်အလှည့်ရောက်အောင်လက်ကလေးပိုက်ပြီးထိုင်စောင့်နေကြတော့မှာလား?။ကျွန်တေ်တို့အောင်လံသစ်ပြန်ထူချင်တယ်။(လူတိုင်းကျန်းမာ၊သက္ကရာဇ်နှစ်ထောင့်တစ်ရာမှာ)ဆိုတဲ့အောင်လံသစ်ကိုအားလုံးဝိုင်းပြီးစိုက်ထူကြရမယ်။ဒီအတွက်ဆရာဝန်တွေကစပြီးလူတန်းစားအားလုံးပါဝင်ဖို့လိုအပ်တယ်။အရင်းရှင်တွေသိမ်းပိုက်ထားတဲ့ကျွန်တော်တို့ရဲ့ကျန်းမာစွာနေထိုင်ခွင့်ကိုကျွန်တော်တို့ပြန်ရယူချင်တယ်။
———
ကျွန်တော်ဒီခေတ်အရင်းရှင်ဆေးပညာကိုဝေဖန်ရေးသားနေတာဟာပုဂ္ဂိုလ်စွဲမဟုတ်သလို၊ဆရာဝန်တွေကိုလဲဝေဖန်ပုတ်ခတ်နေတာမဟုတ်ဘူးဆိုတာကိုတော့ပြတ်ပြတ်သားသားလေးသိစေချင်ပါတယ်။၊ဒီခေတ်ဆေးပညာဟာလူသားတွေအတွက်ကောင်းကျိုးလုံးဝဖြစ်မလာပဲ၊အရင်းရှင်ဆေးကုမ္မဏီကြီးတွေ၊အရင်းရှင်ဆေးရုံဆေးခန်းကြီးတွေကောင်းစားဖို့အတွက်ဖြစ်သွားရတာပါ။အရင်းရှင်စနစ်ဆိုးကြီးဟာအမေရိကန်နိုင်ငံကအစပြုပြီးတကမ္ဘာလုံးမှာကြီးစိုးနေပါပြီ။အခုခေတ်မှာဖြစ်ပွားနေတဲ့ကင်ဆာ၊ဆီးချို၊နှလုံးအစရှိတဲ့ရောဂါတွေကိုအလွယ်ဆုံးနည်းနဲ့ကုန်ကျစရိတ်မရှိပဲကုသလို့ရတဲ့သဘာဝနည်းလမ်းတွေအများကြီးရှိနေပါတယ်။သုသေသနအထောက်အထားတွေလဲအခိုင်အမာရှိနေပါတယ်။ဒါပေမဲ့မိခင်သဘာဝကပေးတဲ့သဘာဝဆေးဝါးတွေကိုဘယ်သူကမှတစ်ဦးတစ်ယောက်တည်းမူပိုင်ခွင့်(Patent)လုပ်ထားလို့မရသလို၊ရောဂါကိုလဲအရှင်းအပြတ်ပျောက်ကင်းသွားစေနိုင်တဲ့အတွက်လူနာကိုလဲရေရှည်နဖားကြိုးတပ်ထားလို့မရနိုင်ပါဘူး။ဒီအကြောင်းနှစ်ချက်ကြောင့်အရင်းရှင်ဆေးကုမ္မဏီကြီးတွေ၊ဆေးရုံဆေးခန်းကြီးတွေကတကယ်ပျောက်ပေမဲ့ပိုက်ဆံကိုရေရှည်ဆွဲပြီးတောင်းလို့မရနိုင်တဲ့သဘာဝနည်းလမ်းတွေကိုလုံးဝစိတ်မဝင်စားကြပါဘူး။
———-
စိတ်မဝင်စားကြတဲ့အပြင်ဒီနည်းလမ်းတွေကိုလူတွေသိကုန်မှာစိုးလို့မီဒီယာတွေကိုသုံး၊ငွေကြေးတွေအကုန်အကျခံပြီးသတင်းမှားတွေဖြန့်လွှင့်၊သုသေသနအလိမ်အညာတွေလုပ်ပြပြီးတော့အကြီးအကျယ်ကိုဖျက်ဆီးတိုက်ခိုက်နေကြပါတယ်။တလောကတောင်(Green Tea)တွေသောက်လို့လူတွေဒုက္ခရောက်ပါတယ်ဆိုပြီးနာမည်ကြီးမီဒီညာတခုကထလုပ်လိုက်သေးတယ်။တစ်ကယ်တန်းလက်တွေ့မှာ(Green Tea)သောက်လို့သေကြေးဆိုရင်ဂျပန်တွေတယောက်မှကိုမကျန်တော့ဘူး။နောက်ပြီး(Vitamin D)သောက်ရင်အကြောတွေခိုင်သွားတဲ့ရောဂါရတတ်တယ်လို့နာမည်ကြီးမီဒီညာတခုကဂျင်းထည့်ပြန်တယ်။(Vitamin D)ကြောင့်အကြောတွေခိုင်ကြေးဆိုရင်၊နေပူထဲမှာအလုပ်လုပ်နေရတဲ့လူတွေပိုလီယိုရောဂါသည်တွေလိုအကြောဆွဲနေတာကြာလှပြီ။မီဒီညာပြောတိုင်းတော့မယုံကြပါနဲ့မိမိအသိဉာဏ်နဲ့အကျိုးအကြောင်းညီညွတ်သလားမညီညွတ်သလားစဉ်းစားကြပေါ့။
———————–
ခေတ်သစ်ဆေးပညာနဲ့ဆရာဝန်တွေကပြောသေးတယ်၊တိရိစ္ဆာန်အဆီတွေ၊ထောပါတ်တွေ၊အုန်းဆီတွေမစားကြနဲ့တဲ့၊အဲဒါတွေကပြည့်ဝဆီတွေတဲ့၊ပြည့်ဝဆီတွေစားလို့(LDL)ကော်လက်စထရောတွေတက်လာပြီးလူတွေနှလုံးရောဂါဖြစ်ကြတာတဲ့။ပြည့်ဝဆီကလာတဲ့(LDL)ကော်လက်စထရောကသိပ်ဆိုးတယ်တဲ့။သူကနှလုံးသွေးကြောတွေမှာပိတ်ပြီးလူတွေနှလုံးရပ်သေကြတာတဲ့။နှလုံးရောဂါဟာကမ္ဘာပေါ်မှာ(၁၉၇၀)နောက်ပိုင်းကစပြီလူတွေအသေအပျောက်တဖြေးဖြေးများလာလို့အခုဆိုရင်နှလုံးရောဂါဟာကမ္ဘာပေါ်မှာအသေအပျောက်အများဆုံးရောဂါတခုဖြစ်လာနေပြီတဲ့။ကော်လက်စထောဟာနှလုံးအတွက်သိပ်ဆိုးစေတယ်ဆိုတဲ့အကြောင်းကိုလဲကော်လက်စထရောကျဆေးထုတ်ရောင်းတဲ့ကုမ္မဏီကြီးတွေကသေသေချာချာသုသေသနတွေလုပ်ပေးထားတဲ့အထောက်အထားတွေအများကြီးရှိနေတယ်တဲ့။မယုံမရှိကြနဲ့တဲ့။ခင်ဗျားတို့ယုံကြလား?ဖြစ်နိုင်လား?
———
ခေါင်းထဲမှာဦးနှောက်ပါတာပဲ၊မိမိအသိဉာဏ်နဲ့အကျိုးအကြောင်းညီညွတ်သလားမညီညွတ်ဘူးလားစဉ်းစားရမှာပေါ့။ကျွန်တော်ပြန်မေးမယ်။ကမ္ဘာဦးတုံးကလူတွေဘာအဆီစားခဲ့ကြလဲ?။အဲဒီလူတွေဟာ(supermarket)တွေမှာဆီကိုပုလင်းတွေနဲ့ဝယ်စားကြတာလား?။အမဲလိုက်လို့ရတဲ့တိရိစ္ဆာန်အဆီ၊နို့ကရတဲ့ထောပါတ်၊အုန်းပင်ကရတဲ့အုန်းဆီစတဲ့ပြည့်ဝဆီတွေပဲစားခဲ့ကြတာမဟုတ်ဘူးလား။ကမ္ဘာဦးကတည်းကပြည့်ဝဆီကလွဲလို့ဘာဆီများတခြားစားစရာရှိလဲ၊အဲဒီရှေးတုံးကလူတွေတယောက်တလေလောက်နှလုံးရောဂါရတယ်။(heart attack)ဖြစ်ပြီးသေကြတယ်ဆိုတာရာဇဝင်တွေထဲဖတ်ဖူးကြားဖူးကြလား။မဟာဇာနကမင်းသားဟာ၊သင်္ဘောပေါ်မှာရသမျှထောပါတ်တွေပြည့်ဝဆီတွေသောက်ပြီးတော့ရွက်တိုင်ထိပ်တက်၊ခုန်ချပြီးတော့သမုဒ္ဒရာထဲမှာ(၇)ရက်ကူးဖြတ်တာကူးနေရင်းနဲ့ပြည့်ဝဆီတွေကြောင့်(Heart attack)ရတယ်ဆိုတာရောကြားဖူးကြလား?။
——–
အမေရိကန်ရဲ့နှလုံးရောဂါကာကွယ်ရေးအဖွဲ့(American Heart association)ကဒီလိုစကားမျိုးကို(၁၉၇၀)နောက်ပိုင်းမှာထုတ်ပြန်ကြေငြာပြီးဂျင်းထည့်လိုက်လို့၊လူတိုင်းတကမ္ဘာလုံးပြည့်ဝဆီကိုကြောက်ပြီးရှောင်လိုက်ကြတယ်။ပြည့်ဝဆီနေရာမှာသကြားကိုပိုစားလာကြတယ်။အဲဒီပြည့်ဝဆီကိုဖြတ်လိုက်တဲ့အချိန်ကစပြီးအခုအချိန်အထိကမ္ဘာပေါ်မှာ(Heart attack)ကြောင့်သေကြရတာသောက်သောက်လဲပါပဲ။အခုတော့နှလုံးရောဂါဟာအသေအပျောက်အများဆုံးရောဂါဖြစ်သွားပြီ။ပြည့်ဝဆီတွေစားလို့သေတာလား။ပြည့်ဝဆီတွေဖြတ်လိုက်လို့သေတာလား။အခုမနေ့တနေ့ကမှစဖြစ်လာတဲ့နှလုံးရောဂါရဲ့တရားခံကိုကမ္ဘာဦးကတည်းကနှစ်ပေါင်းသန်းနဲ့ချီပြီးစားလာတဲ့ဆီကြောင့်ဆိုပြီးတော့စွဲချက်တင်တယ်ဆိုတော့တရားသလား?။အမေရိကန်ရဲ့နှလုံးရောဂါကာကွယ်ရေးအဖွဲ့(American Heart association)ကဒီလိုစကားမျိုးပြောလိုက်တာနှလုံးရောဂါဆေးတွေ၊ကော်လက်စထရောကျဆေးတွေရောင်းတဲ့ဆေးကုမ္မဏီတွေဆီကငွေဘယ်လောက်ရလိုက်သလဲ?။စဉ်းစားစရာပါ။ဒီခေတ်ဆေးပညာဟာယခုအချိန်အထိအဲဒီအဖွဲ့ကြီးရဲ့လမ်းညွန်မှုအတိုင်းဆက်သွားနေတုန်းပါပဲ။
——————-
ပြန်ဆက်မယ်ဗျာ။သဘာဝဆေးဝါးတွေဆိုတာကဘယ်သူမှတစ်ဦးတည်းကိုယ်ပိုင်လုပ်ပြီးလက်ဝါးကြီးအုပ်ထားလို့မရပါဘူး။ဥပမာတခုပေးရရင်မြင်းခွာရွက်ကဘာရောဂါ၊ညာရောဂါတွေပျောက်ပါတယ်လို့ပြောလို့အရင်းရှင်ဆေးကုမ္မဏီကြီးတွေပိုက်ဆံတပြားမှမရနိုင်ဘူး။မြင်းခွာရွက်ကိုလဲငါ့ကုမ္မဏီမူပိုင်လို့လုပ်ထားပြီးတကမ္ဘာလုံးကလူတွေငါ့ကုမ္မဏီရဲ့ခွင့်ပြုချက်မရပဲ၊ငါ့ဆီကမဝယ်ပဲနဲ့ဘယ်သူမှမြင်းခွာရွက်သုံးခွင့်မရှိဘူး၊သုံးရင်တရားစွဲမယ်လို့လုပ်ထားလို့လဲမရဘူး။အရင်းရှင်ဆေးပညာစနစ်ဟာရောဂါအရင်းအမြစ်ကိုပျောက်အောင်မကုပဲရောဂါကနေဖြစ်လာတဲ့အပေါ်ယံလက္ခဏာလေးကိုမှေးပြီးတော့ယာယီကလေးသက်သာနေအောင်လုပ်ထားပြီးမှအောက်ခံရောဂါအစစ်ကိုပိုပိုပြီးဆိုးလာအောင်လောင်စာတွေမီးထိုးပေးထားတော့မှရေရှည်စားရမှာလေ။ဒီတော့အဲဒီလိုဆေးတွေကိုသာတမင်ထွင်လိုက်တယ်။ပြီးရင်တစ်ဦးတည်းမူပိုင်ခွင့်တင်လိုက်တယ်။လူနာတွေကိုရောင်းတယ်။ဆေးကလဲရည်ရွယ်ထားတဲ့အတိုင်းရောဂါရဲ့အပေါ်ယံလက္ခဏာကိုသက်သာစေတယ်။အောက်ခံတကယ့်ရောဂါပိုပိုဆိုးလာတယ်ဆိုတာလူမသိဘူး။အပေါ်ယံလက္ခဏာလေးသက်သာတော့နံမည်လေးရလာတယ်။ဆရာဝန်တွေကိုကော်မရှင်စားပေးထားရင်တော့၊ဆရာဝန်တွေကညွှန်ပေးတော့လက်မလည်အောင်ပိုရောင်းရတယ်။တစ်ယောက်ထဲမူပိုင်ခွင့်လုပ်ထားတော့ပိုက်ဆံအကုန်ကိုပဲရတယ်။ဘယ်ဆေးကုမ္မဏီမှဆေးတလုံးထဲသောက်လိုက်ရုံနဲ့ရောဂါအရှင်းပျောက်တဲ့ဆေးမတီထွင်ဘူး။ခင်ဗျားတို့တီထွင်ပြီးသွားရောင်းရင်လဲသူတို့စိတ်မဝင်စားဘူး။သူတို့စိတ်ဝင်စားတာကရောဂါသက်သာသလိုလိုနဲ့ပိုပြီးရင့်ရင့်၊ဆိုးဆိုးလာတဲ့ဆေး၊တဖြေးဖြေးတိုးတိုးပြီးပိုပိုသောက်လာရမဲ့ဆေး၊ရောဂါမပျောက်ပဲလက္ခဏာလေးပျောက်အောင်ခဏလေးဖုန်းဖိထားပေးမဲ့ဆေး၊မသေမချင်းတသက်လုံးစွဲသောက်ရမယ့်ဆေးကိုပဲစိတ်ဝင်စားကြတာပါ။
—————-
မြဲမြဲမှတ်ထားရမှာကဆေးတခုကိုတိုးတိုးပြီးသောက်နေရတယ်ဆိုကတည်းကအဲဒီဆေးဟာဒီရောဂါကိုပျောက်အောင်ကုပေးမဲ့ဆေးမဟုတ်ဘူးဆိုတာသေချာတယ်။ရောဂါကအရင်ကထက်ပိုပြီးဆိုးဆိုးလာလို့သာဆေးကိုတိုးတိုးသောက်နေရတာပါ၊ရောဂါသာသက်သာသွားမယ်ဆိုရင်တဖြေးဖြေးလျော့လျော့ပြီးသောက်ရမှာပေါ့။နောက်ဆုံးရောဂါပျောက်သွားလို့သောက်စရာတောင်မလိုတော့ဘူးပေါ့။ဆီးချိုဆေးတွေမှာတစ်နေ့ထက်တနေ့လျော့လျော့ပြီးသောက်ရတဲ့ဆေး၊နောက်ဆုံးရောဂါပျောက်သွားလို့၊သောက်စရာမလိုတော့ပဲဖြတ်လိုက်ရတဲ့ဆေးမျိုးရှိလား?။ရှိရင်ညွန်ပေးကြပါဗျာ၊ကျွန်တော်လဲဝယ်ထားချင်လို့ပါ။အခုခေတ်မှာကျန်းမာရေးအတွက်ဆေးပညာဆိုတာမရှိတော့ပါဘူး၊စီးပွါးရေးအတွက်ဆေးပညာဖြစ်သွားပါပြီ။လူတိုင်းလူတိုင်းကျန်းမာရေးဗဟုသုတရှိမှသာအသက်ရှည်ကျန်းမာနိုင်ပါမယ်။ဒီစကားတွေကိုမယုံရင်တော့နောင်တကောင်းကောင်းရပါလိမ့်မယ်။ဒါပေမဲ့ဒီဘဝမှာတော့ရမှာမဟုတ်ဘူး၊နောင်ဘဝကြမှနောင်တရပါလိမ့်မယ်။
————————
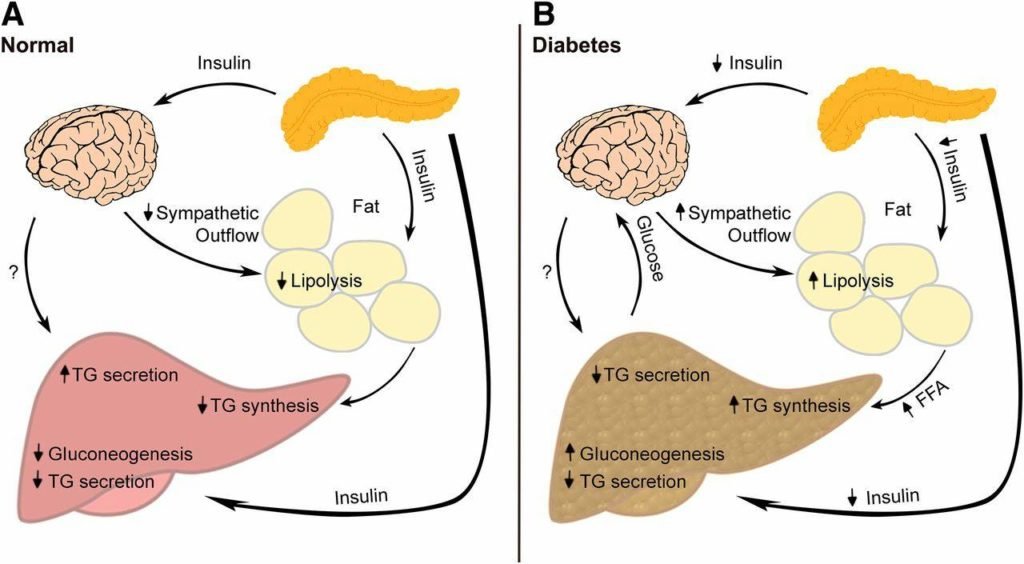
Type-2 Diabetes)အကြောင်းဆက်ပါဦးမယ်။အပိုင်း(၃)မှာတုံးကပြောထားတဲ့အတိုင်းဒီရောဂါနဲ့ဆက်စပ်နေတဲ့အသဲရဲ့ပင်မလမ်းကြောင်းကြီးလေးခုထဲက၊နံပါတ်(၁)ဖြစ်တဲ့(hepatic gluconeogenesis pathways)လို့ခေါ်တဲ့အသဲကနေသကြားဓါတ်ဂလူးကို့စ်(Glucose)ထုတ်ပေးနေတဲ့လမ်းကြောင်းအကြောင်းကိုဆက်ပြီးလေ့လာကြည့်ကြပါစို့။(Type-2 Diabetes)သမားတစ်ယောက်ဟာအိပ်ခါနီးသွေးဖေါက်တိုင်းကြည့်တော့သွေးထဲမှာလဲသကြားဓါတ်ကသိပ်အမြင့်ကြီးတက်မနေဘူး။အိပ်ရာမဝင်ခင်မှာလဲဘာမှမစားပဲနဲ့အိပ်ရာဝင်လိုက်တယ်။နောက်နေ့မနက်အိပ်ရာကနိုးတော့လဲဘာမှမစားခင်(Fasting)အချိန်မှာသွေးဖေါက်ပြီးဂလူးကို့စ်တိုင်းကြည့်တော့ အရမ်းမြင့်တက်နေတယ်ဆိုရင်မဖြစ်မနေလုပ်ရမှာကအစာမစားခင်မနက်စောစောဓါတ်ခွဲခန်းတခုသွားပြီး(fasting Insulin)ကိုတိုင်းတာရပါမယ်။မြန်မာပြည်မှာ(fasting Insulin)တိုင်းပေးတဲ့(lab)တွေအများကြီးရှိနေပါပြီ။
————— (၁)မိမိကိုယ်တိုင်သေချာတိုင်းကြည့်ထားတာဂလူးကိုယ့်စ်ဟာမိမိဘာမှထပ်မစားပဲညကထက်မနက်ပိုင်းမှာပိုပြီးမြင့်တက်နေတယ်။အပြင်ကသကြားဓါတ်လာတာမဟုတ်ပဲနဲ့မိမိအသဲကသာသကြားထုတ်လုပ်ပေးနေပြီး၊ထုတ်လုပ်မှုကိုရပ်တန့်သင့်တဲ့အချိန်မှာမရပ်တန့်နိုင်လို့သာမနက်ပိုင်းသွေးထဲမှာသကြားဓါတ်တွေတက်နေတာပါလား။
(၂)ဘာမှမစားခင်အင်ဆူလင်တိုင်းကြည့်တော့လဲမိမိသွေးထဲမှာလဲအင်ဆူလင်ကလဲမြင့်တက်နေပြန်တယ်။ဒီလိုဆိုတော့ပန်ကရိယကပျက်စီးနေတာမဟုတ်လို့သာအင်ဆူလင်ကိုလုံလောက်စွာထုတ်ပေးနေနိုင်တာကတော့သေချာနေပြီ။သို့သော်ထုတ်ထားပေးတဲ့အင်ဆူလင်တွေကသွေးထဲမှာအများကြီးရှိနေရက်သားနဲ့၊အသဲကအင်ဆူလင်ရဲ့စကားကိုနားမထောင်ပဲသကြားထုတ်လုပ်မှု့ကိုမရပ်တန့်နိုင်ပဲဆက်လုပ်နေတာဟာငါ့အသဲမှာအင်ဆူလင်ခုခံမှု(hepatic insulin resistant)ဆိုတဲ့ရောဂါဖြစ်နေတယ်ဆိုတာသေချာနေပါလား။
—————-
တကယ်တော့ဆီးချိုရောဂါဆိုတာမရှိပါလား။သွေးထဲမှာသကြားဓါတ်များနေတဲ့လက္ခဏာဆိုတာကလဲငါ့အသဲမကောင်းလို့အသဲကပုံမှန်အလုပ်မလုပ်နိုင်လို့သာသကြားဓါတ်ထုတ်လုပ်မှု့ကိုမရပ်တန့်ပြစ်နိုင်လို့ဖြစ်လာရတဲ့ရောဂါရဲ့လက္ခဏာပါလားဆိုပြီးအကြောင်းတရားကြောင့်ဖြစ်လာရတဲ့အကျိုးတရားဆိုတာကိုတိတိကျကျသိရပါတော့မယ်။သိတယ်ဆိုတာကလဲသူများကလာပြောပြလို့သိရတာလဲမဟုတ်ဘူး။ဆရာဝန်ပြောလို့သိရတာလဲမဟုတ်ဘူး၊စာအုပ်ထဲမှာရေးထားလို့သိရတာလဲမဟုတ်ဘူး။အပြင်မှာလက်တွေ့မိမိကိုယ်တိုင်တိုင်းကြည့်လို့သိလိုက်ရတာ။ဒီထက်ခိုင်မာတဲ့အရာဆိုတာမရှိနိုင်တော့ပါဘူး။အကျိုးအကြောင်းတွေအားလုံးညီညွတ်နေပြီဆိုတော့ဒီနေရာမှာဆုံးဖြတ်ချက်ပြုတ်ပြုတ်သားသားချနိုင်ဖို့ပဲလိုအပ်ပါတော့တယ်။ဘယ်လိုဆုံးဖြတ်ရမလဲဆိုတော့၊ငါဖြစ်နေတာကအသဲရောဂါ၊ငါကုနေတာကသွေးထဲကသကြားဓါတ်၊ငါ့ဆရာဝန်ပေးနေတဲ့ဆေးတွေကလဲအသဲကျန်းမာလာအောင်ကုတဲ့ဆေးတခုမှမပါဘူး။ငါနဲ့ငါ့ဆရာဝန်နဲ့ငါအတူတကွကြိုးစားနေတာကသွေးထဲမှာရှိတဲ့သကြားဓါတ်ကျဆင်းရေး၊ဒါဟာရောဂါကိုမကုပဲရောဂါကဖြစ်ပေါ်လာတဲ့လက္ခဏာသက်သက်ကိုထိုင်ကုနေကြပါလားဆိုတာသေချာသိကိုသိရတော့မယ်။
————————–
ဒီနေရာမှာသွေးထဲမှာရှိတဲ့သကြားဓါတ်ကိုကျအောင်မလုပ်ကြပါနဲ့လို့ကျွန်တော်လုံးဝလုံးဝမဆိုလိုပါဘူး။သကြားဓါတ်တက်နေတာဟာအလွန်အန္တရာယ်များပါတယ်။ရေတိုလေးမှာတော့သကြားဓါတ်ကျအောင်တော့လုပ်ကိုလုပ်ရပါမယ်။ဒါပေမဲ့ရေရှည်ကောင်းစေချင်ရင်တော့အသဲကိုအဓိကဦးစားပေးပြီးကုသရပါမယ်။အခုခေတ်ဆေးပညာမှာလုံးဝမှားယွင်းနေတာကဆီးချိုရောဂါသည်တွေကိုဆရာဝန်တွေကအသဲကိုအဓိကထားပြီးကုတယ်ဆိုတာမရှိပါဘူး။သွေးထဲမှာသကြားဓါတ်လေးကျသွားရေးကိုသာနည်းအမျိုးမျိုး၊ဆေးအမျိုးမျိုးသုံးပြီးကျိုးစားနေကြတာပါ။ဒီလိုကုလို့ကတော့ဘယ်တော့မှမပျောက်နိုင်တဲ့အပြင်ကြာလေပိုဆိုးလာလေပါပဲ။အပိုင်း(၁)မှာရေးထားသလိုမိုက်မဲတဲ့ထင်းခုတ်သမားဟာသစ်ပင်ကိုမခုတ်ပဲအရိပ်ကိုသာထိုင်ခုတ်နေသလိုဖြစ်မနေဘူးလားဆိုတာသေချာစဉ်းစားကြည့်ပါ။ခွေးကိုခဲနဲ့ပေါက်လိုက်ရင်ခွေးကခဲလုံးကိုစိတ်ဆိုးပြီးဒေါတတကြီးနဲ့လိုက်ကိုက်တတ်တယ်။ခြင်္သေ့ကိုခဲနဲ့ပေါက်လိုက်ရင်တော့ခြင်္သေ့ဟာခဲလုံးကိုဘယ်တော့မှလိုက်မကိုက်ဘူး။ခဲဘယ်ကလာတာလဲ၊ဘယ်သူပြစ်လွတ်တာလဲဆိုတာသေချာစူးစမ်းတယ်။ငါ့ရန်သူဟာခဲလုံးတော့မဟုတ်ဘူး၊ပြစ်တဲ့လူကိုရှာရမယ်ဆိုတာကိုသေချာနားလည်တယ်။
———-
အခုလဲဒီဥပမာလိုပဲ၊(type-2 Diabetes)ဟာအသဲကြောင့်ဖြစ်နေတာကိုမသိတော့မိမိကိုတကယ်ဒုက္ခပေးနေတဲ့အသဲရောဂါကိုပြစ်မှတ်ထားပြီးမကုပဲနဲ့ထိုရောဂါရဲ့လက္ခဏာသက်သက်ဖြစ်နေတဲ့သွေးထဲမှာတက်နေတဲ့သကြားဓါတ်တခုတည်းကိုပဲမကျကျအောင်ဆေးအမျိုးမျိုးတွေသောက်၊အင်ဆူလင်တွေထိုးသွင်းနေတာဟာခဲလုံးကိုလိုက်ကိုက်နေတာနဲ့တူနေသလား၊ဒါမှမဟုတ်ပညာရှိတဲ့ခြင်္သေ့နဲ့တူနေသလားဆိုတာကိုကိုယ်တိုင်ဆုံးဖြတ်ကြည့်ကြပါ။ဒါကိုတိတိကျကျသိတော့မှမိမိကိုယ်တိုင်၊ဒီကနေ့ကစပြီးတောငါ့အသဲကိုသာငါအဓိကပြစ်မှတ်ထားပြီးကုတော့မယ်လို့ခိုင်ခိုင်မာမာဆုံးဖြတ်ချက်ချနိုင်မှာဖြစ်တယ်။ဒီလိုဆုံးဖြတ်ချက်ချနိုင်တဲ့နေ့ဟာမိမိမှာရှိနေတဲ့ဆီးချိုရောဂါကိုပျောက်အောင်ကုသနိုင်ဖို့(၉၀%)လောက်သေချာသွားတဲ့နေ့လို့သတ်မှတ်လိုက်ပါ။အနာသိမှတော့ဆေးရှိပါတယ်။အနာမသိလို့သာဒုက္ခရောက်နေကြရတာပါ။
————————–
အသဲကိုအဓိကထားကုသရတော့မယ်ဆိုတော့၊အသဲအကြောင်းကိုဆက်ပြီးလေ့လာကြရအောင်။အသဲကဘာလို့အင်ဆူလင်ခိုင်းတာကိုမလုပ်ရတာလဲ။ဘာလို့မလိုက်နာပဲဆန့်ကျင်နေရတာလဲ။အသဲနဲ့အင်ဆူလင်ကြားမှာသဟဇာတမဖြစ်တာဘာများရှိနေလို့လဲ။ဒီအဖြေကိုရှာမှကိုရမှာပါ။ဒီအဖြေကိုမသိရင်ဒီအသဲကိုဘယ်လိုကုသနိုင်မှာလဲ။အကျိုးရှိရင်အကြာင်းရှိရမယ်။အကြောင်းသိရင်အဖြေရှိရမယ်။အင်ဆူလင်ဆိုတာဘာလဲ။အင်ဆူလင်ခုခံမှု့ဆိုတာကရောဘာလဲ၊ဘာကြောင့်ဖြစ်လာရတာလဲဆိုတာဆက်ပြီးအသေးစိတ်လေ့လာကြရအောင်။ဒီနေ့တော့ရေးတာနဲနဲလေးများသွားပြီးခေါင်းစဉ်အောက်ကနေလဲဘေးကိုနဲနဲလေးတော့ထွက်သွားတယ်။ဒါပေမဲ့မသိထားတဲ့ဗဟုသုတသစ်တွေကိုသိလိုက်ရတော့အသုံးဝင်အကျိုးရှိကြမှာပါ။နားဦးမယ်ဗျာ။နောက်နေ့မှဆက်ရေးပါမယ်။
—————————-
Kelvin Albert Power
————————References———————-
1. Ekberg K, et al. Contributions by kidney and liver to glucose production in the postabsorptive state and after 60 h of fasting. Diabetes. 1999;48:292–298. [PubMed] [Google Scholar]
2. Moore MC, Coate KC, Winnick JJ, An Z, Cherrington AD. Regulation of hepatic glucose uptake and storage in vivo. Adv Nutr. 2012;3:286–294. [PMC free article] [PubMed] [Google Scholar]
3. Rizza RA. Pathogenesis of fasting and postprandial hyperglycemia in type 2 diabetes: implications for therapy. Diabetes. 2010;59:2697–2707. [PMC free article] [PubMed] [Google Scholar]
4. Moore MC, et al. Sources of carbon for hepatic glycogen synthesis in the conscious dog. J Clin Invest. 1991;88:578–587. [PMC free article] [PubMed] [Google Scholar]
5. Rothman DL, Magnusson I, Katz LD, Shulman RG, Shulman GI. Quantitation of hepatic glycogenolysis and gluconeogenesis in fasting humans with 13C NMR. Science. 1991;254:573–576. [PubMed] [Google Scholar]
6. Mari A, Wahren J, DeFronzo RA, Ferrannini E. Glucose absorption and production following oral glucose: comparison of compartmental and arteriovenous-difference methods. Metabolism. 1994;43:1419–1425. [PubMed] [Google Scholar]
7. Ishida T, et al. Differential effects of oral, peripheral intravenous, and intraportal glucose on hepatic glucose uptake and insulin and glucagon extraction in conscious dogs. J Clin Invest. 1983;72:590–601. [PMC free article] [PubMed] [Google Scholar]
8. Pagliassotti MJ, Cherrington AD. Regulation of net hepatic glucose uptake in vivo. Annu Rev Physiol. 1992;54:847–860. [PubMed] [Google Scholar]
9. Ferrannini E, et al. The disposal of an oral glucose load in healthy subjects A quantitative study. Diabetes. 1985;34:580–588. [PubMed] [Google Scholar]
10. Petersen KF, Laurent D, Rothman DL, Cline GW, Shulman GI. Mechanism by which glucose and insulin inhibit net hepatic glycogenolysis in humans. J Clin Invest. 1998;101:1203–1209. [PMC free article] [PubMed] [Google Scholar]
11. Lin HV, Accili D. Hormonal regulation of hepatic glucose production in health and disease. Cell Metab. 2011;14:9–19. [PMC free article] [PubMed] [Google Scholar]
12. Cherrington AD, Edgerton D, Sindelar DK. The direct and indirect effects of insulin on hepatic glucose production in vivo. Diabetologia. 1998;41:987–996. [PubMed] [Google Scholar]
13. Pagliassotti MJ, Moore MC, Neal DW, Cherrington AD. Insulin is required for the liver to respond to intraportal glucose delivery in the conscious dog. Diabetes. 1992;41:1247–1256. [PubMed] [Google Scholar]
14. McGuinness OP, Ayala JE, Laughlin MR, Wasserman DH. NIH experiment in centralized mouse phenotyping: the Vanderbilt experience and recommendations for evaluating glucose homeostasis in the mouse. Am J Physiol Endocrinol Metab. 2009;297:E849–E855. [PMC free article] [PubMed] [Google Scholar]
15. Kowalski GM, Bruce CR. The regulation of glucose metabolism: implications and considerations for the assessment of glucose homeostasis in rodents. Am J Physiol Endocrinol Metab. 2014;307:E859–E871. [PubMed] [Google Scholar]
16. Steele R, et al. Inhibition by insulin of hepatic glucose production in the normal dog. Am J Physiol. 1965;208:301–306. [PubMed] [Google Scholar]
17. Rizza RA, Mandarino LJ, Gerich JE. Dose–response characteristics for effects of insulin on production and utilization of glucose in man. Am J Physiol. 1981;240:E630–E639. [PubMed] [Google Scholar]
18. Basu A, Shah P, Nielsen M, Basu R, Rizza RA. Effects of type 2 diabetes on the regulation of hepatic glucose metabolism. J Investig Med. 2004;52:366–374. [PubMed] [Google Scholar]
19. Magnusson I, Rothman DL, Katz LD, Shulman RG, Shulman GI. Increased rate of gluconeogenesis in type II diabetes mellitus. A 13C nuclear magnetic resonance study. J Clin Invest. 1992;90:1323–1327. [PMC free article] [PubMed] [Google Scholar]
20. Perry RJ, Samuel VT, Petersen KF, Shulman GI. The role of hepatic lipids in hepatic insulin resistance and type 2 diabetes. Nature. 2014;510:84–91. [PMC free article] [PubMed] [Google Scholar]
21. Kumashiro N, et al. Cellular mechanism of insulin resistance in nonalcoholic fatty liver disease. Proc Natl Acad Sci USA. 2011;108:16381–16385. [PMC free article] [PubMed] [Google Scholar]
22. Petersen KF, et al. Reversal of nonalcoholic hepatic steatosis, hepatic insulin resistance, and hyperglycemia by moderate weight reduction in patients with type 2 diabetes. Diabetes. 2005;54:603–608. [PMC free article] [PubMed] [Google Scholar]
23. Petersen KF, et al. Leptin reverses insulin resistance and hepatic steatosis in patients with severe lipodystrophy. J Clin Invest. 2002;109:1345–1350. [PMC free article] [PubMed] [Google Scholar]
24. Perry RJ, Zhang D, Zhang X-M, Boyer JL, Shulman GI. Controlled-release mitochondrial protonophore reverses diabetes and steatohepatitis in rats. Science. 2015;347:1253–1256. [PMC free article] [PubMed] [Google Scholar]
25. Perry RJ, et al. Reversal of hypertriglyceridemia, fatty liver disease, and insulin resistance by a liver-targeted mitochondrial uncoupler. Cell Metab. 2013;18:740–748. [PMC free article] [PubMed] [Google Scholar]
26. Kim JK, Gavrilova O, Chen Y, Reitman ML, Shulman GI. Mechanism of insulin resistance in A-ZIP/F-1 fatless mice. J Biol Chem. 2000;275:8456–8460. [PubMed] [Google Scholar]
27. Samuel VT, Shulman GI. Mechanisms for insulin resistance: common threads and missing links. Cell. 2012;148:852–871. [PMC free article] [PubMed] [Google Scholar]
28. Magkos F, et al. Intrahepatic diacylglycerol content is associated with hepatic insulin resistance in obese subjects. Gastroenterology. 2012;142:1444–1446 e2. [PMC free article] [PubMed] [Google Scholar]
29. Luukkonen PK, et al. Hepatic ceramides dissociate steatosis and insulin resistance in patients with nonalcoholic fatty liver disease. J Hepatol. 2016;64:1167–1175. [PubMed] [Google Scholar]
30. ter Horst KW, et al. Hepatic diacylglycerol-associated protein kinase Cε translocation links hepatic steatosis to hepatic insulin resistance in humans. Cell Rep. 2017;19:1997–2004. [PMC free article] [PubMed] [Google Scholar]
31. Samuel VT, et al. Inhibition of protein kinase Cε prevents hepatic insulin resistance in nonalcoholic fatty liver disease. J Clin Invest. 2007;117:739–745. [PMC free article] [PubMed] [Google Scholar]
32. Samuel VT, et al. Mechanism of hepatic insulin resistance in non-alcoholic fatty liver disease. J Biol Chem. 2004;279:32345–32353. [PubMed] [Google Scholar]
33. Petersen MC, et al. Insulin receptor Thr1160 phosphorylation mediates lipid-induced hepatic insulin resistance. J Clin Invest. 2016;126:4361–4371. [PMC free article] [PubMed] [Google Scholar]
34. Michelotti GA, Machado MV, Diehl AM. NAFLD, NASH and liver cancer. Nat Rev Gastroenterol Hepatol. 2013;10:656–665. [PubMed] [Google Scholar]
35. Williams AS, et al. Integrin-linked kinase is necessary for the development of diet-induced hepatic insulin resistance. Diabetes. 2017;66:325–334. [PMC free article] [PubMed] [Google Scholar]
36. Boden G. Gluconeogenesis and glycogenolysis in health and diabetes. J Investig Med. 2004;52:375–378. [PubMed] [Google Scholar]
37. Chen X, Iqbal N, Boden G. The effects of free fatty acids on gluconeogenesis and glycogenolysis in normal subjects. J Clin Invest. 1999;103:365–372. [PMC free article] [PubMed] [Google Scholar]
38. Katz J, Tayek JA. Gluconeogenesis and the Cori cycle in 12-, 20-, and 40-h-fasted humans. Am J Physiol. 1998;275:E537–E542. [PubMed] [Google Scholar]
39. Landau BR, et al. Contributions of gluconeogenesis to glucose production in the fasted state. J Clin Invest. 1996;98:378–385. [PMC free article] [PubMed] [Google Scholar]
40. Levine R, Fritz IB. The relation of insulin to liver metabolism. Diabetes. 1956;5:209–219. [PubMed] [Google Scholar]
41. Gaisano H, MacDonald PE, Vranic M. Glucagon secretion and signaling in the development of diabetes. Front Physiol. 2012;3:349. [PMC free article] [PubMed] [Google Scholar]
42. Pearson MJ, Unger RH, Holland WL. Clinical trials, triumphs, and tribulations of glucagon receptor antagonists. Diabetes Care. 2016;39:1075–1077. [PMC free article] [PubMed] [Google Scholar]
43. Ader M, Bergman RN. Peripheral effects of insulin dominate suppression of fasting hepatic glucose production. Am J Physiol. 1990;258:E1020–E1032. [PubMed] [Google Scholar]
44. Lewis GF, Zinman B, Groenewoud Y, Vranic M, Giacca A. Hepatic glucose production is regulated both by direct hepatic and extrahepatic effects of insulin in humans. Diabetes. 1996;45:454–462. [PubMed] [Google Scholar]
45. Sindelar DK, Balcom JH, Chu CA, Neal DW, Cherrington AD. A comparison of the effects of selective increases in peripheral or portal insulin on hepatic glucose production in the conscious dog. Diabetes. 1996;45:1594–1604. [PubMed] [Google Scholar]
46. Prager R, Wallace P, Olefsky JM. Direct and indirect effects of insulin to inhibit hepatic glucose output in obese subjects. Diabetes. 1987;36:607–611. [PubMed] [Google Scholar]
47. Staehr P, et al. Effects of free fatty acids per se on glucose production, gluconeogenesis, and glycogenolysis. Diabetes. 2003;52:260–267. [PubMed] [Google Scholar]
48. Lewis GF, Vranic M, Harley P, Giacca A. Fatty acids mediate the acute extrahepatic effects of insulin on hepatic glucose production in humans. Diabetes. 1997;46:1111–1119. [PubMed] [Google Scholar]
49. Sindelar DK, et al. The role of fatty acids in mediating the effects of peripheral insulin on hepatic glucose production in the conscious dog. Diabetes. 1997;46:187–196. [PubMed] [Google Scholar]
50. Rebrin K, Steil GM, Mittelman SD, Bergman RN. Causal linkage between insulin suppression of lipolysis and suppression of liver glucose output in dogs. J Clin Invest. 1996;98:741–749. [PMC free article] [PubMed] [Google Scholar]
51. Perry RJ, et al. Hepatic acetyl coa links adipose tissue inflammation to hepatic insulin resistance and type 2 diabetes. Cell. 2015;160:745–758. [PMC free article] [PubMed] [Google Scholar]
52. Perry RJ, et al. Leptin reverses diabetes by suppression of the hypothalamic–pituitary–adrenal axis. Nat Med. 2014;20:759–763. [PMC free article] [PubMed] [Google Scholar]
53. Perry RJ, Peng L, Shulman GI. Mechanism for leptin’s acute insulin-independent effect to reverse diabetic ketoacidosis. J Clin Invest. 2017;127:657–669. [PMC free article] [PubMed] [Google Scholar]
54. Previs SF, Cline GW, Shulman GI. A critical evaluation of mass isotopomer distribution analysis of gluconeogenesis in vivo. Am J Physiol. 1999;277:E154–E160. [PubMed] [Google Scholar]
55. Krebs HA, Speake RN, Hems R. Acceleration of renal gluconeogenesis by ketone bodies and fatty acids. Biochem J. 1965;94:712–720. [PMC free article] [PubMed] [Google Scholar]
56. Keech DB, Utter MF. Pyruvate carboxylase. II Properties. J Biol Chem. 1963;238:2609–2614. [PubMed] [Google Scholar]
57. Williamson JR, Kreisberg RA, Felts PW. Mechanism for the stimulation of gluconeogenesis by fatty acids in perfused rat liver. Proc Natl Acad Sci USA. 1966;56:247–254. [PMC free article] [PubMed] [Google Scholar]
58. Lu M, et al. Insulin regulates liver metabolism in vivo in the absence of hepatic Akt and Foxo1. Nat Med. 2012;18:388–395. [PMC free article] [PubMed] [Google Scholar]
59. Buettner C, et al. Severe impairment in liver insulin signaling fails to alter hepatic insulin action in conscious mice. J Clin Invest. 2005;115:1306–1313. [PMC free article] [PubMed] [Google Scholar]
60. Okamoto H, Obici S, Accili D, Rossetti L. Restoration of liver insulin signaling in Insr knockout mice fails to normalize hepatic insulin action. J Clin Invest. 2005;115:1314–1322. [PMC free article] [PubMed] [Google Scholar]
61. Chen YD, Golay A, Swislocki AL, Reaven GM. Resistance to insulin suppression of plasma free fatty acid concentrations and insulin stimulation of glucose uptake in noninsulin-dependent diabetes mellitus. J Clin Endocrinol Metab. 1987;64:17–21. [PubMed] [Google Scholar]
62. Fraze E, et al. Ambient plasma free fatty acid concentrations in noninsulin-dependent diabetes mellitus: evidence for insulin resistance. J Clin Endocrinol Metab. 1985;61:807–811. [PubMed] [Google Scholar]
63. Reaven GM, Hollenbeck C, Jeng CY, Wu MS, Chen YD. Measurement of plasma glucose, free fatty acid, lactate, and insulin for 24 h in patients with NIDDM. Diabetes. 1988;37:1020–1024. [PubMed] [Google Scholar]
64. Golay A, Swislocki AL, Chen YD, Reaven GM. Relationships between plasma-free fatty acid concentration, endogenous glucose production, and fasting hyperglycemia in normal and non-insulin-dependent diabetic individuals. Metabolism. 1987;36:692–696. [PubMed] [Google Scholar]
65. Swislocki AL, Chen YD, Golay A, Chang MO, Reaven GM. Insulin suppression of plasma-free fatty acid concentration in normal individuals and patients with type 2 (non-insulin-dependent) diabetes. Diabetologia. 1987;30:622–626. [PubMed] [Google Scholar]
66. Charles MA, et al. The role of non-esterified fatty acids in the deterioration of glucose tolerance in Caucasian subjects: results of the Paris Prospective Study. Diabetologia. 1997;40:1101–1106. [PubMed] [Google Scholar]
67. Paolisso G, et al. A high concentration of fasting plasma non-esterified fatty acids is a risk factor for the development of NIDDM. Diabetologia. 1995;38:1213–1217. [PubMed] [Google Scholar]
68. Jocken JWE, et al. Insulin-mediated suppression of lipolysis in adipose tissue and skeletal muscle of obese type 2 diabetic men and men with normal glucose tolerance. Diabetologia. 2013;56:2255–2265. [PMC free article] [PubMed] [Google Scholar]
69. Heptulla RA, et al. In situ evidence that peripheral insulin resistance in adolescents with poorly controlled type 1 diabetes is associated with impaired suppression of lipolysis: a microdialysis study. Pediatr Res. 2003;53:830–835. [PubMed] [Google Scholar]
70. Gelding SV, Coldham N, Niththyananthan R, Anyaoku V, Johnston DG. Insulin resistance with respect to lipolysis in non-diabetic relatives of European patients with type 2 diabetes. Diabet Med. 1995;12:66–73. [PubMed] [Google Scholar]
71. Robinson C, et al. Effect of insulin on glycerol production in obese adolescents. Am J Physiol. 1998;274:E737–E743. [PubMed] [Google Scholar]
72. Puhakainen I, Koivisto VA, Yki-Järvinen H. Lipolysis and gluconeogenesis from glycerol are increased in patients with noninsulin-dependent diabetes mellitus. J Clin Endocrinol Metab. 1992;75:789–794. [PubMed] [Google Scholar]
73. Nurjhan N, Consoli A, Gerich J. Increased lipolysis and its consequences on gluconeogenesis in non-insulin-dependent diabetes mellitus. J Clin Invest. 1992;89:169–175. [PMC free article] [PubMed] [Google Scholar]
74. Perry RJ, Peng L, Cline GW, Petersen KF, Shulman GIA. Non-invasive method to assess hepatic acetyl-CoA in vivo. Cell Metab. 2017;25:749–756. [PMC free article] [PubMed] [Google Scholar]
75. American Diabetes Association. 7. Approaches to glycemic treatment. Diabetes Care. 2016;39:S52–S59. [PubMed] [Google Scholar]
76. Hundal RS, et al. Mechanism by which metformin reduces glucose production in type 2 diabetes. Diabetes. 2000;49:2063–2069. [PMC free article] [PubMed] [Google Scholar]
77. Inzucchi SE, et al. Efficacy and metabolic effects of metformin and troglitazone in type II diabetes mellitus. N Engl J Med. 1998;338:867–872. [PubMed] [Google Scholar]
78. Zhou G, et al. Role of AMP-activated protein kinase in mechanism of metformin action. J Clin Invest. 2001;108:1167–1174. [PMC free article] [PubMed] [Google Scholar]
79. Shaw RJ, et al. The kinase LKB1 mediates glucose homeostasis in liver and therapeutic effects of metformin. Science. 2005;310:1642–1646. [PMC free article] [PubMed] [Google Scholar]
80. He L, et al. Metformin and insulin suppress hepatic gluconeogenesis through phosphorylation of CREB binding protein. Cell. 2009;137:635–646. [PMC free article] [PubMed] [Google Scholar]
81. Fullerton MD, et al. Single phosphorylation sites in Acc1 and Acc2 regulate lipid homeostasis and the insulin-sensitizing effects of metformin. Nat Med. 2013;19:1649–1654. [PMC free article] [PubMed] [Google Scholar]
82. Foretz M, et al. Metformin inhibits hepatic gluconeogenesis in mice independently of the LKB1/AMPK pathway via a decrease in hepatic energy state. J Clin Invest. 2010;120:2355–2369. [PMC free article] [PubMed] [Google Scholar]
83. Madiraju AK, et al. Metformin suppresses gluconeogenesis by inhibiting mitochondrial glycerophosphate dehydrogenase. Nature. 2014;510:542–546. [PMC free article] [PubMed] [Google Scholar]
84. Cao J, et al. Low concentrations of metformin suppress glucose production in hepatocytes through AMP-activated protein kinase (AMPK) J Biol Chem. 2014;289:20435–20446. [PMC free article] [PubMed] [Google Scholar]
85. Hawley SA, Gadalla AE, Olsen GS, Hardie DG. The antidiabetic drug metformin activates the AMP-activated protein kinase cascade via an adenine nucleotide-independent mechanism. Diabetes. 2002;51:2420–2425. [PubMed] [Google Scholar]
86. Howell JJ, et al. Metformin inhibits hepatic mTORC1 signaling via dose-dependent mechanisms involving AMPK and the TSC complex. Cell Metab. 2017;25:463–471. [PMC free article] [PubMed] [Google Scholar]
87. El-Mir MY, et al. Dimethylbiguanide inhibits cell respiration via an indirect effect targeted on the respiratory chain complex I. J Biol Chem. 2000;275:223–228. [PubMed] [Google Scholar]
88. Hardie DG, Ross FA, Hawley SA. AMPK: a nutrient and energy sensor that maintains energy homeostasis. Nat Rev Mol Cell Biol. 2012;13:251–262. [PMC free article] [PubMed] [Google Scholar]
89. Miller RA, et al. Biguanides suppress hepatic glucagon signalling by decreasing production of cyclic AMP. Nature. 2013;494:256–260. [PMC free article] [PubMed] [Google Scholar]
90. Konopka AR, et al. Hyperglucagonemia mitigates the effect of metformin on glucose production in prediabetes. Cell Rep. 2016;15:1394–1400. [PMC free article] [PubMed] [Google Scholar]
91. Pernicova I, Korbonits M. Metformin — mode of action and clinical implications for diabetes and cancer. Nat Rev Endocrinol. 2014;10:143–156. [PubMed] [Google Scholar]
92. Brown LJ, et al. Normal thyroid thermogenesis but reduced viability and adiposity in mice lacking the mitochondrial glycerol phosphate dehydrogenase. J Biol Chem. 2002;277:32892–32898. [PubMed] [Google Scholar]
93. Saheki T, et al. Citrin/mitochondrial glycerol-3-phosphate dehydrogenase double knock-out mice recapitulate features of human citrin deficiency. J Biol Chem. 2007;282:25041–25052. [PubMed] [Google Scholar]
94. Baur JA, Birnbaum MJ. Control of gluconeogenesis by metformin: does redox trump energy charge? Cell Metab. 2014;20:197–199. [PMC free article] [PubMed] [Google Scholar]
95. Exton JH, Park CR. Control of gluconeogenesis in liver. II. Effects of glucagon, catecholamines, and adenosine 3′,5′-monophosphate on gluconeogenesis in the perfused rat liver. J Biol Chem. 1968;243:4189–4196. [PubMed] [Google Scholar]
96. Lee Y, et al. Hyperglycemia in rodent models of type 2 diabetes requires insulin-resistant alpha cells. Proc Natl Acad Sci USA. 2014;111:13217–13222. [PMC free article] [PubMed] [Google Scholar]
97. Blair JB, Cimbala MA, Foster JL, Morgan RA. Hepatic pyruvate kinase. Regulation by glucagon, cyclic adenosine 3′-5′-monophosphate, and insulin in the perfused rat liver. J Biol Chem. 1976;251:3756–3762. [PubMed] [Google Scholar]
98. Rider MH, et al. 6-Phosphofructo-2-kinase/ fructose-2,6-bisphosphatase: head-to-head with a bifunctional enzyme that controls glycolysis. Biochem J. 2004;381:561–579. [PMC free article] [PubMed] [Google Scholar]
99. Wu C, et al. Perturbation of glucose flux in the liver by decreasing F26P2 levels causes hepatic insulin resistance and hyperglycemia. Am J Physiol Endocrinol Metab. 2006;291:E536–E543. [PubMed] [Google Scholar]
100. Cullen KS, Al-Oanzi ZH, O’Harte FPM, Agius L, Arden C. Glucagon induces translocation of glucokinase from the cytoplasm to the nucleus of hepatocytes by transfer between 6-phosphofructo 2-kinase/fructose 2,6-bisphosphatase-2 and the glucokinase regulatory protein. Biochim Biophys Acta. 2014;1843:1123–1134. [PMC free article] [PubMed] [Google Scholar]